You don't have to test everyone, every day. You have to be able to test people the moment they feel something, and provide them with answers in a very short timeframe. If they return a positive, they then have to have their friends and those they came in contact with tested. If they return a negative, they carry on. If they return a positive, they isolate and tell those they were in contact with...and so on.
It's not perfect, but it will release a large portion of the population who isn't infected out into the world without assuming everyone else is a spreader.
We need to be testing like no country has ever tested in the history of the world. The testing will be amazing, because we have the smartest people in the world...it'll be fantastic how much testing we'll do. No other administration ever tested like we'll be testing. When we get there...we'll be in much better shape than we are today.
We already know that many get infected and can transmit, yet feel nothing and never know they were infected.
You don't have to test everyone, every day. You have to be able to test people the moment they feel something, and provide them with answers in a very short timeframe. If they return a positive, they then have to have their friends and those they came in contact with tested. If they return a negative, they carry on. If they return a positive, they isolate and tell those they were in contact with...and so on.
It's not perfect, but it will release a large portion of the population who isn't infected out into the world without assuming everyone else is a spreader.
We need to be testing like no country has ever tested in the history of the world. The testing will be amazing, because we have the smartest people in the world...it'll be fantastic how much testing we'll do. No other administration ever tested like we'll be testing. When we get there...we'll be in much better shape than we are today.
There is no meaningful testing for this virus unless everyone is tested everydaybefore they leave their home to go outside and interact with the world. We do not yet know that having had the virus and recovering means you are immune or no longer a carrier.
Everything else is just being delusional, playing whack a mole because of how quickly things can change. You can just go outside and never see anyone, yet touch something that someone who was positive touched and get infected that way.
I have to ask: if there is statistically significant evidence that fewer Covid19 patients are dying or that more of them are recovered/discharged, does that serve as hard evidence that the coronavirus's virulence is decreasing, or that medical groups are becoming more effective at treating Covid19?
I think it's really premature to call the peak of coronavirus infections and deaths.
Stop - right - there. I called it a trend. I referred to the change of direction as a peak, yet it is only a trend. A trend is defined as a general direction in which something is developing or changing and nothing more. Trends are things that are changing and fleeting and can be short lived. Yet they are recognizable as an entity that can be measured.
I thought that it was a good thing to recognize, this measurable change in direction. There are actual numbers. Will it last ? I dunno, but it is the first sign of things actually improving where there has been none before now. Sure there are always mitigating circumstances, but it is nice to recognize an improvement in the overall outlook once in a while, imho.
So go ahead and be a Debbie Downer; there never is any good news in your world.
have a dreary day ... if that is what makes you happy.
There is no really good news yet. We've been locked away for 6 to 8 weeks, and we're finally seeing the numbers go down in many areas. If we stay inside forever the virus will go away, but luckily for us there are well-armed peopled working to ensure we're liberated.
The best news of the day may be from todays NYTimes, which reported that in Boston, NY, San Fran, Chicago and Seattle as of March 1 there were only 23 confirmed cases of coronavirus. Based on a new model by Northeastern, there could have actually been about 28,000 infections in those cities by then. Sure would be nice to have anti-body testing.
In order to be able to control outbreaks and return to a bit of normalcy, we need to be testing beyond our capabilities at this point. The stat that people should be looking at is Positivity Rate.
According to the Tracking Projectâs figures, nearly one in five people who get tested for the coronavirus in the United States is found to have it. In other words, the country has what is called a âtest-positivity rateâ of nearly 20 percent...
...The test-positivity rate, then, is a decent (if unusual) proxy for the severity of an outbreak in an area. And it shows clearly that the U.S. still lags far behind other countries in the course of fighting its outbreak. South Korea â which discovered its first coronavirus caseon the same day as the U.S. â has tested more than half a million people, or about 1 percent of its population, and discovered about 10,500 cases. The U.S. has now tested 3.2 million people, which is also about 1 percent of its population, but it has found more than 630,000 cases. So while the U.S. has a 20 percent positivity rate, South Koreaâs is only about 2 percent â a full order of magnitude smaller.
South Korea is not alone in bringing its positivity rate down: Americaâs figure dwarfs that of almost every other developed country. Canada, Germany and Denmark have positivity rates from 6 to 8 percent. Australia and New Zealand have 2 percent positivity rates. Even Italy â which faced one of the worldâs most ravaging outbreaks â has a 15 percent rate. It has found nearly 160,000 cases and conducted more than a million tests. Virtually the only wealthy country with a larger positivity rate than the U.S. is the United Kingdom, where more than 30 percent of people tested for the virus have been positive...
The article is a week old now....we're down to 18.5% in the US. at this rate, we'll be ready to roll in about 8 to 10 weeks.
I've been watching these trends and they are finally beginning to reverse. .
CLOSED CASES
928,844
Cases which had an outcome:
739,971 (80%)
Recovered / Discharged
188,873 (20%)
Deaths
It was down to 79% and 21% (the peak) respectively for several weeks.
ACTIVE CASES
1,769,677
Currently Infected Patients
1,711,657 (97%)
in Mild Condition
58,020 (3%)
Serious or Critical
Previously it was 95% and 5% (also the peak) respectively for the same several weeks.
++++++++++ THIS IS NOT ME ARGUING ++++++++++
I do worry about "the other shoe," however
US: CLOSED CASES 133,919
Cases which had an outcome: 84,825 (63%)Recovered / Discharged 49,094 (37%)Deaths
Coronavirus Cases: 868,482
I know the 37% deaths out of all cases which had an outcome will drop. To 20%, the worldwide number right now? That's still 20% of 868,000. I hope I'm mis-reading the charts.
I have to ask: if there is statistically significant evidence that fewer Covid19 patients are dying or that more of them are recovered/discharged, does that serve as hard evidence that the coronavirus's virulence is decreasing, or that medical groups are becoming more effective at treating Covid19?
I think it's really premature to call the peak of coronavirus infections and deaths. I don't recall seeing statements from people trained in medicine and/or epidemiology that the lethality of the coronavirus is decreasing. It doesn't seem that medical personnel have yet found ways to widely and effectively treat Covid19. And we will have more infections when we start to open up the country or parts of the country again.
In fact, we could be facing a much larger second wave of Covid19 infections which if coinciding with flu infections could overwhelm our medical systems.
âThereâs a possibility that the assault of the virus on our nation next winter will actually be even more difficult than the one we just went through,â CDC Director Robert Redfield said in an interview with The Washington Post. âAnd when Iâve said this to others, they kind of put their head back, they donât understand what I mean.â
âWeâre going to have the flu epidemic and the coronavirus epidemic at the same time,â he said.
Having two simultaneous respiratory outbreaks would put unimaginable strain on the health-care system, he said. The first wave of covid-19, the disease caused by the coronavirus, has already killed more than 42,000 people across the country. It has overwhelmed hospitals and revealed gaping shortages in test kits, ventilators and protective equipment for health-care workers.
It also seems that it's difficult to get a firm understanding of how lethal the Coronavirus is. See the article quoted below: since most people with mild cases won't get tested for Coronavirus, the number of actual cases is likely underreported and the ratio of deaths to infections exaggerated. And given the days-to-weeks lag between infection and death, "current death rates should properly be divided by the number of known infections from the previous week or two" (from article excerpt below). More widespread testing for Covid19 will drive the reported death rate down but adjusting calculations for the time delay between infections and deaths will drive the reported death rate up.
ALSOâas the CDC director implied (see above), a large increase in Covid19 cases combined an increase in flu infections could overwhelm our hospitals and drive up death rates.
How deadly is the new coronavirus? The death rate from the novel coronavirus that causes the COVID-19 disease varies by location, age of person infected and the presence of underlying health conditions.
While most people who catch the new coronavirus SARS-CoV-2 recover at home, some may need hospitalization to fight the virus. And in a number of patients, COVID-19 is deadly.
Scientists can't yet say for sure what the fatality rate of the coronavirus is, because they're not certain how many people have become infected with the disease. But they do have some estimates, and there is a widespread consensus that COVID-19 is most dangerous for elderly patients and those with preexisting health burdens.
On March 5, Tedros Adhanom Ghebreyesus, director-general of the World Health Organization, said during a news conference that about 3.4% of reported COVID-19 patients around the world have died. In aChinese analysis of more than 72,000 case records, 2.3% of those confirmed or suspected (based on symptoms and exposure) to have the virus died. Patients above 80 years of age had an alarmingly high fatality rate of 14.8%. Patients ages 70 to 79 years had a fatality rate of 8% and those ages 60 to 69 had a fatality rate of 3.6%. (Younger age groups had lower fatality rates; 1.3% for those 50 to 59; 0.4% for the age group 40 to 49; and just 0.2% for people ages 10 to 39.) In Italy, which has a high proportion of residents over age 65, the fatality rate is strikingly high, around 10% as of March 25.
A recent study of COVID-19 cases in the United States estimated a mortality rate of 10% to 27% for those ages 85 and over, 3% to 11% for those ages 65 to 84, 1% to 3% for those ages 55 to 64 and less than 1% for those ages 20 to 54.
These numbers shouldn't be taken as the inevitable toll of the virus, however. The case-fatality rate is determined by dividing the number of deaths by the total number of cases. Epidemiologists believe the total number of infections with SARS-CoV-2 is underestimated because people with few or mild symptoms may never see a doctor. As testing expands and scientists begin using retrospective methods to study who has antibodies to SARS-CoV-2 circulating in their bloodstreams, the total number of confirmed cases will go up and the ratio of deaths to infections will likely drop.
For example, in South Korea, which conducted more than 140,000 tests for COVID-19, officials found a fatality rate of 0.6%.
However, complicating the matter, mortality numbers lag behind infection numbers simply because it takes days to weeks for severely ill people to die of COVID-19. Thus, current death rates should properly be divided by the number of known infections from the previous week or two, researchers wrote in February inSwiss Medical Weekly.
A report published March 13 in the journal Emerging Infectious Diseasesadjusted for this "time delay" between hospitalization and death. The authors estimated that, as of Feb. 11, the death rate from COVID-19 was as high as 12% in Wuhan, 4% in Hubei Province and 0.9% in the rest of China.
Another factor affecting the deadliness of the new coronavirus is the quality of medical care. Already, there is evidence that the overwhelmed medical system in Wuhan, where the outbreak began, led to more deaths.The World Health Organization's joint mission report from Feb. 28 found that among 56,000 laboratory-confirmed coronavirus cases, the case-fatality ratio was 3.8%. However, the case-fatality ratio in Wuhan was 5.8%, while the rest of the country â spared the overwhelming bulk of sick patients â saw a rate of 0.7%.
This means fewer people are likely to die if the medical system is prepared to face an influx of coronavirus patients.
Indeed, in the Emerging Infectious Diseases report, the authors said that the high death rate estimates for Wuhan "are probably associated with a breakdown of the healthcare system," which was overwhelmed with cases. The findings indicate that "enhanced public health interventions, including social distancing and movement restrictions, should be implemented to bring the COVID-19 epidemic under control," the authors said.
Cases which had an outcome: 84,825 (63%)Recovered / Discharged 49,094 (37%)Deaths
Coronavirus Cases: 868,482
I know the 37% deaths out of all cases which had an outcome will drop. To 20%, the worldwide number right now? That's still 20% of 868,000. I hope I'm mis-reading the charts.
No worries.
I do not have a date stamp but kept an old window open when there were 500,879 total cases.
At that time the total recovered was 27,239 and the total deaths was 18,637 for a closed case total of 45,876 which works out to about 60% to 40% ±. So that ratio is also improving.
So just for the sake of discussion purposes, these are the trends to watch as the country reopens.
I've been watching these trends and they are finally beginning to reverse. .
CLOSED CASES
928,844
Cases which had an outcome:
739,971 (80%)
Recovered / Discharged
188,873 (20%)
Deaths
It was down to 79% and 21% (the peak) respectively for several weeks.
ACTIVE CASES
1,769,677
Currently Infected Patients
1,711,657 (97%)
in Mild Condition
58,020 (3%)
Serious or Critical
Previously it was 95% and 5% (also the peak) respectively for the same several weeks.
++++++++++ THIS IS NOT ME ARGUING ++++++++++
I do worry about "the other shoe," however
US: CLOSED CASES 133,919
Cases which had an outcome: 84,825 (63%)Recovered / Discharged 49,094 (37%)Deaths
Coronavirus Cases: 868,482
I know the 37% deaths out of all cases which had an outcome will drop. To 20%, the worldwide number right now? That's still 20% of 868,000. I hope I'm mis-reading the charts.
Um, you're confusing the physical diameter of an object with the distance between peaks of a wave (frequency) of a visible colored beam of light.
Not the same.
The resolution of an optical microscope is about half the wavelength of the light illuminating the specimen. Resolution is the distance two objects have to be apart in order to be seen as distinct (separate) objects. Here's a good article on the topic.
We use scanning electron microscopy to see really tiny details as the wavelength of an electron is way smaller than visible light. But SEMs come with limitations: if you just hose down a non-conductive object (like, say, a cell or virus) with electrons it will build up electrostatic charge and interfere with the image. That's why most specimens are coated with something conductive, like carbon or gold. Since you need a clear path between the electron source, the object, and the detector the imaging is done in a vacuum chamber to avoid air molecules interfering with the beams and images. These limitations mean anything you're seeing in a normal SEM image is dead.
There is a technique for imaging things at higher pressures (not a hard vacuum) called Environmental SEM. Still pretty rare, hoping to learn more about it. Looks promising.
SEMs are also slow. A single frame can take many minutes.
There are specialized techniques to improve optical resolution, like confocal microscopy, that rely on fluorescence. Very useful for viewing biological processes in 3D. Don't think they could see any detail at Covid-19 scale.
More than 21% of the New York City residents given coronavirus antibody tests earlier this week tested positive, Gov. Andrew Cuomo said Thursday. Monday marked the start of a statewide initiative to test 3,000 New Yorkers for the presence of antibodies, which are made in response to viral infections. The preliminary results mean that one in five of the city residents tested have had coronavirus and developed the antibodies to fight it. Across the state, 13.9% of the individuals tested were positive for antibodies, Cuomo told reporters at a daily news briefing. New York state is the epicenter of the U.S. outbreak of the novel coronavirus that causes COVID-19, with more than 250,000 cases and more than 19,000 fatalitie
For reference, there are about 8.4m in NYC and almost 20m in the state.
"if we can't get film of the virus invading a host cell and replicating, then how do we know?" We do have such film. I saw clips of such activity while watching the excellent series on PBS, "The Gene: An Intimate History."
I think that guy on FB needs to use the vast resources of the Internet to read up and educate himself.
You said you wanted film, as in moving pictures. You could hit it with x-rays but they'll blow right thru. You could hit it with electron beams but that requires a vacuum and carbon sputtering over the sample, and besides the scan rate is ridiculously slow. You'll get still images of dead cells and viruses.
There are techniques for pushing the resolution limit but 125 nm is going to be (at best) a speck, no detail.
If you've got something I don't know about I'm all ears.
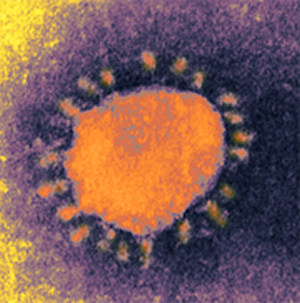
Human coronavirus 229E. The same image as above, but colorized. Negative contrast electron microscopy. Classical negative contrast images of coronaviruses are really not the way they look when in their native state. The peplomers (spikes) fall off so easily that most images seen in atlases and textbooks are really partly "bald," as are these. Native virions are actually so heavily covered with peoplmers that virions might not be recognized if only the classical images are in mind. Magnification approximately x60,000.
Micrograph from F. A. Murphy, University of Texas Medical Branch, Galveston, Texas.
You might be able to use scanning electron microscopy to capture an image of the surface of the virus, perhaps: . https://blog.phenom-world.com/...
Again, the PBS series "The Gene: An Intimate History" that I watched showed a series of images, at the very least much like a movie if not a movie itself, of a virus injecting material into a cell.
I take film as a colloquialism for imagery, but anyway, back in my student days we took photographs to capture the images from the scanning electron microscope where the resolution is (checks google) ~10 nm. I believe there was a translation step of exciting phosphors with the scattered electrons but still counts in my book.
Then there are things like atomic force microscopy where you can image down to the atomic level but you might not consider that to be pictures.
And before AFM there was Field Ion Microscopy. You can image individual atoms under some circumstances. My first job as an undergrad in metallurgy school was in a FIM lab.
And I apologize, it wasn't you but kcar who wanted '"...film of the virus invading a host cell and replicating"', but that implies a moving image, which ain't gonna happen.
You said you wanted film, as in moving pictures. You could hit it with x-rays but they'll blow right thru. You could hit it with electron beams but that requires a vacuum and carbon sputtering over the sample, and besides the scan rate is ridiculously slow. You'll get still images of dead cells and viruses.
There are techniques for pushing the resolution limit but 125 nm is going to be (at best) a speck, no detail.
If you've got something I don't know about I'm all ears.
I take film as a colloquialism for imagery, but anyway, back in my student days we took photographs to capture the images from the scanning electron microscope where the resolution is (checks google) ~10 nm. I believe there was a translation step of exciting phosphors with the scattered electrons but still counts in my book.
Then there are things like atomic force microscopy where you can image down to the atomic level but you might not consider that to be pictures.
You said you wanted film, as in moving pictures. You could hit it with x-rays but they'll blow right thru. You could hit it with electron beams but that requires a vacuum and carbon sputtering over the sample, and besides the scan rate is ridiculously slow. You'll get still images of dead cells and viruses.
There are techniques for pushing the resolution limit but 125 nm is going to be (at best) a speck, no detail.
If you've got something I don't know about I'm all ears.